
Most enterprise buyers now demand evidence of real security before they sign. Without operational controls and continuous proof, deals stall, and healthcare vendors face the sharpest scrutiny over who can touch patient data. HIPAA least privilege is the practice of granting each user, program, or system only the access strictly required to do its job. That single discipline shrinks your attack surface and directly supports the minimum necessary standard at the heart of the HIPAA Privacy Rule. In this guide, we show you how to design PHI access controls that stand up to buyers, auditors, and attackers. The patterns here come from supporting 6,000+ audits over 25+ years of combined experience, where human-led managed security delivers outcomes that documents alone never can. Controls that look good on paper but fail under incident pressure are a liability. Build durable ones instead.
What Is Least Privilege and How It Relates to HIPAA
The principle of least privilege dictates that a user, program, or system process should hold only the bare minimum access privileges needed to perform its intended function. In a healthcare context, that means a billing specialist gets access to financial records and specific billing codes but zero access to a patient's full psychiatric history. By restricting access rights, organizations sharply reduce the surface area for data breaches, insider threats, and accidental exposure of sensitive health information.
Mapped to healthcare regulation, this concept directly supports the minimum necessary standard, which requires covered entities to evaluate their practices and tighten safeguards that limit unnecessary access to protected health information (PHI). Achieving least privilege under HIPAA keeps your organization aligned with these federal mandates while actively protecting patient confidentiality. Authorized data access becomes a deliberate, engineered process rather than a default assumption.
Many teams confuse least privilege with a strict need-to-know basis. Need-to-know asks whether a person requires specific data for a specific task; least privilege is the technical boundary that enforces that restriction automatically. Together they create a defense-in-depth approach. We implement these controls inside your stack, so that when an auditor reviews your environment, the evidence matches your stated policies.
The Enterprise Reality: Why Buyers Demand Proof
When you sell into healthcare or enterprise environments, buyers send rigorous security questionnaires, Business Associate Agreements (BAAs), and Data Processing Agreements (DPAs). Procurement teams no longer accept promises. They demand verified evidence of an operational Information Security Management System (ISMS). The evidence that blocks or accelerates deals usually centers on how well you control access to electronic protected health information (ePHI) and sensitive corporate data. With breaches involving a third party increasing 68% in 2024, enterprise procurement teams scrutinize your supply chain risk and internal access policies heavily.
Being audit-ready means having continuous evidence across an observation period, not a snapshot. Evidence generation alone is insufficient; you need real control implementation. Buyers want to see change-management records, active access reviews, vendor risk workflows, and vulnerability management tracked against strict service-level agreements (SLAs).
We see the difference in timelines constantly. Typical SOC 2 Type II readiness takes 4 to 5 months with Konfirmity versus 9 to 12 months when teams attempt a self-managed approach. The resource burden shifts drastically too. Our end-to-end managed service asks about 75 hours per year from your internal team, compared with the 550 to 600 hours typically consumed by self-managed compliance software. We do not just advise, we execute. By mapping risks across ISO 27001, SOC 2, HIPAA, and GDPR, we enable cross-framework reuse that accelerates enterprise sales cycles.
Why HIPAA Least Privilege Matters in Healthcare
Risk reduction is the primary driver for strict access boundaries. Healthcare environments are prime targets for ransomware and data extortion. The IBM Cost of a Data Breach Report put the average healthcare breach recovery at $9.77 million, the highest of any industry for 14 consecutive years. The AICPA also requires logical access control under the SOC 2 Trust Services Criteria (CC6.1 through CC6.8). When you restrict permissions, you limit the damage an attacker can do if they compromise a single employee's credentials. Least privilege isolates sensitive databases, so a compromised administrative account does not hand over full access to patient medical histories.
Data access control also curbs breaches caused by internal curiosity or negligence. If an employee lacks the technical ability to export a database of ePHI, the risk of accidental disclosure drops toward zero. Technical safeguards enforce policy automatically and remove human error from the equation.
From a compliance view, enforcing these boundaries helps satisfy both federal requirements and independent audits. The Department of Health and Human Services (HHS) and the Office for Civil Rights (OCR) expect organizations to implement the access control standard of the HIPAA Security Rule, which allows access only to those persons or software programs granted access rights. The field results confirm it: organizations that run strict access matrices see fewer unauthorized-access incidents and report cleaner findings during surveillance audits.
The Connection Between Least Privilege and the Minimum Necessary Standard
The minimum necessary standard, set out under 45 CFR 164.502(b) and 164.514(d), requires covered entities to make reasonable efforts to limit the use and disclosure of PHI to the minimum amount needed to accomplish the intended purpose. The intent is to protect patient privacy without impeding care. The rule forces organizations to evaluate their data flows and decide exactly who needs access to what.
Least privilege supplies the technical architecture to enforce that rule. If the minimum necessary standard is the legal mandate, restricted access configurations are the implementation. You define the minimum necessary data for each job role, then configure your systems to enforce those exact boundaries.
Exceptions exist. For treatment purposes, clinicians typically require broad access to medical records to deliver safe, effective care, and the rule does not stop medical professionals from viewing full patient histories when diagnosing or treating individuals. The exceptions are narrow, though. Billing departments, IT support, and external vendors fall squarely under minimum necessary constraints. Mapping these distinct requirements is the foundation of a defensible security program.
Design PHI access controls that hold up under audit and attack.
Drop your work email and we'll map your roles to a least-privilege access matrix that passes buyer scrutiny.
Step-by-Step Implementation Guide
Moving from theoretical policy to technical reality takes a systematic approach, and the controls have to live inside your infrastructure. Here is how we build programs that stand up to regulatory scrutiny.
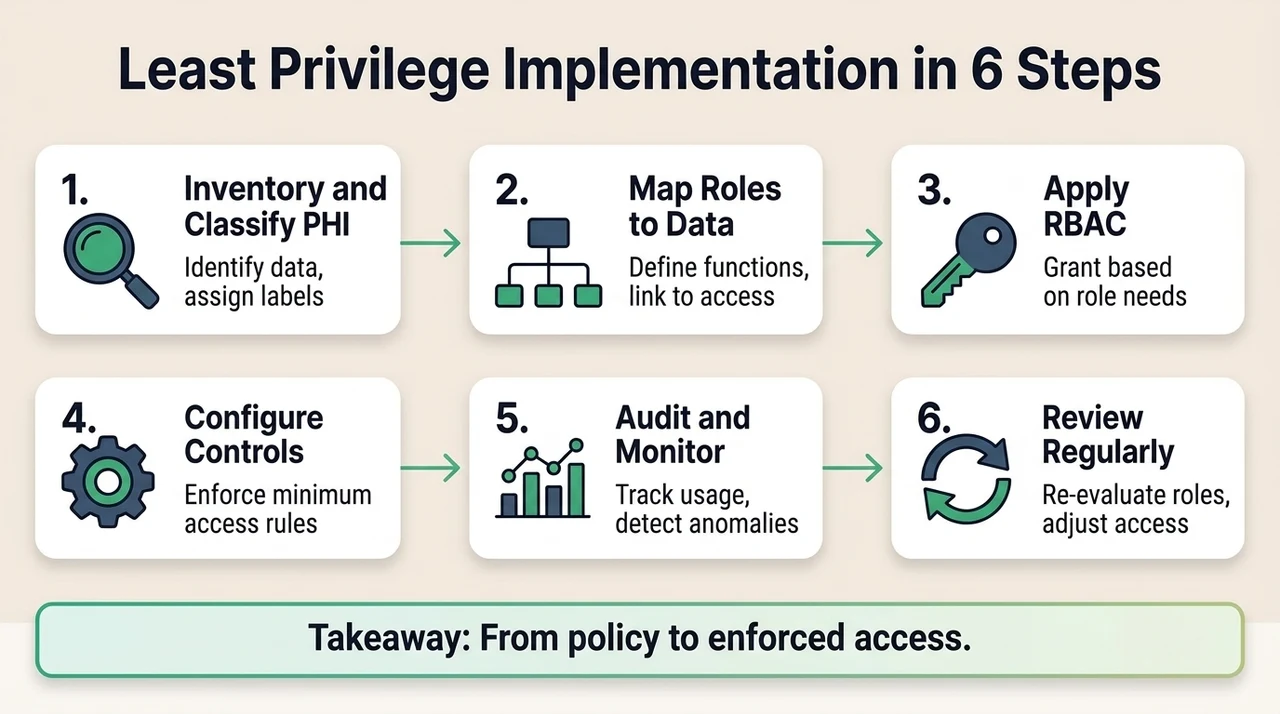
Step 1: Inventory and Classify PHI
Before you can restrict access, you have to locate the data. Document every system, cloud environment, and local server where ePHI is stored, transmitted, or processed. That includes AWS S3 buckets, PostgreSQL databases, SaaS applications, and third-party vendor systems. Tag sensitive fields and workflows so you know what access is genuinely needed. Data minimization matters here: if you do not need to store a specific piece of health data, delete it. Less data means less risk.
Step 2: Map Roles to Data Needs
Define the specific roles in your organization, such as clinicians, nursing staff, billing specialists, system administrators, and third-party vendors. For each role, list exactly what ePHI they need to view or modify, and justify the reason. Create an official access control matrix. This matrix is the source of truth for all provisioning and serves as a primary evidence document during an ISO 27001:2022 or SOC 2 Type II audit.
Step 3: Apply Role-Based Access Control (RBAC)
Use role-based access control to tie user privilege management directly to job responsibilities. Instead of assigning permissions to individual users, assign permissions to a role, then assign users to that role. This keeps provisioning consistent and prevents configuration drift. Enforcing least privilege across your infrastructure depends on strict adherence to this model. Include policies for temporary or exception access, commonly known as break-glass procedures, for emergency medical situations where standard restrictions might endanger a patient. For a deeper walkthrough, see our guide to HIPAA role-based access control.
Step 4: Configure Technical Controls
Enforce data access control through secure authentication. Issue unique user IDs to every individual so that all system actions are accountable. Require multi-factor authentication (MFA) across all endpoints and applications. Configure strict session limits that automatically log out unattended workstations. Use automated provisioning tools to enforce policy and reduce manual error, so that when a user changes roles, the system revokes old permissions and grants new ones based on the updated RBAC profile. Our roundup of HIPAA access control best practices covers the configuration details.
Step 5: Audit, Monitor, and Log Continuously
Set up centralized log management to track all access events, including successful logins, failed attempts, and data export actions. Use logs to detect anomalies and gaps in privilege assignments. Continuous monitoring is a requirement for both HIPAA and SOC 2 Type II. Establish vulnerability management with Common Vulnerability Scoring System (CVSS) based triage and strict remediation SLAs. If an unauthorized user tries to reach a restricted database, your security operations team should get an immediate alert. See our guide to HIPAA logging and monitoring for how to build this out.
Step 6: Review and Adjust Permissions Regularly
Run periodic privilege reviews. We advise quarterly access reviews for all systems that contain ePHI, and monthly reviews for highly privileged administrative accounts. Remove outdated or unnecessary access immediately on employee termination or role change. Evidence of these access reviews is mandatory during an observation period. Without documented reviews, an auditor will issue a non-conformity finding, delaying certification and potentially stalling enterprise sales.
Common Challenges and How to Handle Them
Operational reality tends to complicate security initiatives. What breaks in the field usually comes from poorly designed processes rather than technology failures.
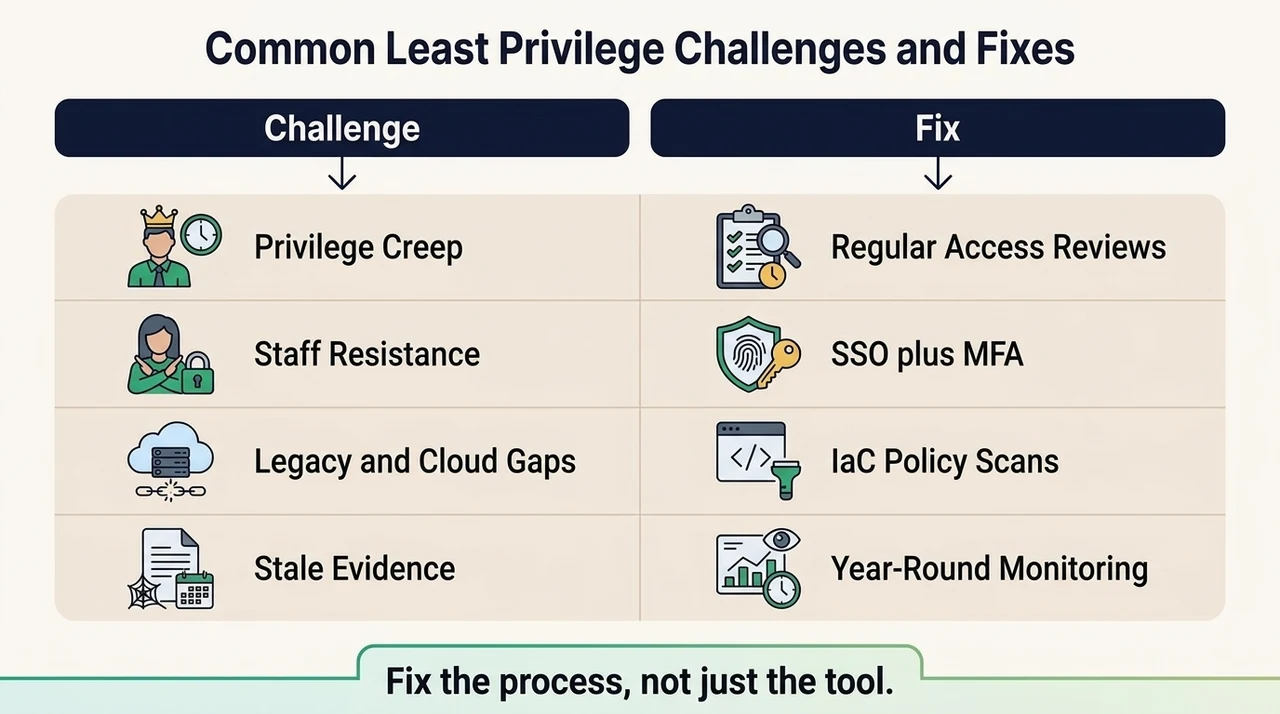
1. Privilege creep. Users accumulate new permissions as they change roles, keep the old ones, and end up with excessive rights across multiple systems. Left unchecked, it is one of the biggest drivers of internal healthcare data breaches. The cause is usually manual provisioning instead of automated, role-based lifecycle management. The fix is to run regular, documented access reviews that reverify the necessity of every permission.
2. Staff resistance and perceived inconvenience. Medical and administrative staff may complain that strict authentication slows their workflows, driven by friction and password fatigue. Address it with clear communication that explains how security protects both patients and the organization's financial viability, and by combining single sign-on (SSO) with MFA to reduce fatigue while keeping strong access boundaries.
3. Integrating restricted access with cloud modernization. Legacy applications often lack granular permission settings and offer only broad "user" or "admin" profiles, while cloud migrations invite misconfigured Identity and Access Management (IAM) policies that inadvertently expose ePHI. Use automated policy checks and infrastructure-as-code scanning to keep controls accurate and prevent deployment errors.
4. Evidence staleness during observation windows. Point-in-time GRC tooling can give a false sense of security when the underlying configuration has drifted, producing an audit failure behind a green checkmark. Human-led managed security keeps configurations matched to policy year-round, tracks remediation, and prevents vendor sprawl.
Durable Practices for Healthcare Organizations
Security that rests entirely on an annual audit check is fundamentally flawed. Controls have to be embedded into daily operations.
Bake restrictive access into your security policies and staff onboarding. From day one, employees should understand that their access is limited by design. Link privacy and IT teams so technical configurations match operational reality; a disconnect between the compliance officer and the engineering team produces policies that look good on paper but do not exist in the infrastructure. Train staff on why controlled access protects patients, making security a shared responsibility rather than an IT obstacle.
Connect risk assessment and governance to your access reviews. During the annual risk assessment required by the HIPAA Security Rule or ISO 27001:2022, evaluate whether your current RBAC matrix still mitigates the threats you have identified. Build Data Protection Impact Assessment (DPIA) triggers into your software development lifecycle, so that whenever engineering proposes a feature that processes ePHI, a DPIA evaluates the access implications before code reaches production.
Least privilege is continuous effort, not a one-time project. Build your program around durable controls rather than evidence generation. Start with security, implement the safeguards inside your stack, and arrive at compliance as a natural result of operational maturity.
Case Studies and Real-World Examples
Real-world patterns show how control design prevents catastrophic breaches. Across our audit-support history, the difference between companies with theoretical security and those with operational security is stark.
Defeating Privilege Creep in a Scaling SaaS Company
A mid-sized healthcare technology provider faced an upcoming SOC 2 Type II audit and a barrage of enterprise procurement questionnaires. Their internal audit revealed severe privilege creep: developers retained production database access long after finishing specific troubleshooting tasks. They implemented a strict RBAC matrix, integrated it with their identity provider, and established automated quarterly access reviews. Three months later, a phishing attack compromised a developer's credentials. Because that developer no longer held standing access to the ePHI databases, the attacker gained nothing. Least privilege turned a potential disaster into a minor, contained incident.
Handling Third-Party Vendor Risk and BAA Gaps
A clinical analytics firm used a third-party vendor for data visualization. The initial integration granted the vendor broad API access to read the entire patient database, violating the minimum necessary standard. During a readiness assessment, we identified the BAA gap and the control failure. The firm restructured the API to expose only anonymized, aggregated data sets required for the visualization tools. When the vendor later suffered a security breach, the analytics firm was unaffected, because the exposed API credentials could only reach sanitized data. It is a clean illustration of why continuous monitoring and third-party risk management are core to a defensible posture.
Tools and Technologies That Support Controlled Access
Software alone does not build a security program, but specific technologies are needed to enforce policy at scale.
Identity and Access Management (IAM) platforms are the central hub for authentication and authorization. Solutions such as Okta, Microsoft Entra ID, or AWS IAM let organizations enforce MFA, manage SSO, and automate user provisioning from HR system triggers. Privileged Access Management (PAM) solutions handle the most sensitive administrative credentials, enforcing strict checkout procedures and recording sessions for database administrators.
Auditing and reporting systems centralize logs from across the infrastructure. A Security Information and Event Management (SIEM) tool aggregates those logs so security teams can detect anomalies and track access patterns.
Buying a tool is not the same as having a security program. Self-serve GRC software pushes hundreds of internal hours onto your engineering team to configure, map, and maintain evidence. Automated provisioning helps enforce least privilege, but human experts have to design the underlying architecture, map controls to regulatory frameworks, and run the ongoing operations. Outcome as a service means we build the program, manage the tools, and deliver audit readiness without draining your internal resources.
Conclusion
Securing healthcare data is an ongoing operational requirement, not a one-time fix. Regulatory frameworks demand continuous governance, rigorous control implementation, and active monitoring, and human-led managed security supplies the technical depth and operational consistency to meet them.
Build durable policies, review your access matrices regularly, and monitor infrastructure continuously. Do not settle for compliance manufacturing that produces paper without technical substance. Implement real controls inside your tech stack. Security that reads well in a document but fails in practice introduces massive risk. Build the program once, operate it daily, and let compliance follow.
FAQ
What exactly is HIPAA least privilege?
It is the practice of restricting a user's access rights to the minimum permissions required to perform their specific job functions. That technical constraint limits exposure of electronic protected health information (ePHI) and reduces the attack surface for potential breaches.
How is it different from role-based access control?
Role-based access control (RBAC) is a mechanism for assigning permissions based on job roles. Least privilege is the broader security philosophy that dictates what those RBAC permissions should actually be. RBAC is how you enforce the philosophy.
Does the regulation require it?
Yes, indirectly, through the minimum necessary standard in the Privacy Rule and the access control specifications in the Security Rule. The law requires covered entities to implement technical policies and procedures for electronic information systems that maintain ePHI, allowing access only to those persons or software programs granted access rights.
What happens if we do not enforce these restrictions?
Failing to enforce strict boundaries introduces severe compliance risk, sharply increases breach likelihood, and produces critical audit findings. During enterprise sales cycles, a lack of operational access controls will lead buyers to reject your security posture, stalling or losing the deal.
How often should we review settings?
We advise documented access reviews quarterly for all systems containing sensitive patient data, and monthly for highly privileged administrative accounts. Reviews should also happen immediately on any employee termination or significant role change.
Can vendors and third-party systems have restricted access?
Yes. Strict permission boundaries apply across all business associates and integrated software systems, not just internal human users. Third-party risk management means evaluating vendor integrations and ensuring that APIs or service accounts hold only the exact data access they need to function.



