
Most enterprise buyers now request assurance artifacts before they sign. Without operational security and continuous evidence, deals stall, even when your team believes it is ready on paper. When healthcare technology companies pitch to hospital systems, procurement departments enforce strict supply chain due diligence. If your organization relies on external software to process patient data, your attack surface expands into systems you do not own. That reality makes HIPAA vendor risk mapping a hard requirement for modern healthcare operations, not a nice-to-have.
Defined in practical terms, HIPAA vendor risk mapping is the structured practice of identifying, categorizing, and continuously tracking the security posture of every third party that touches patient data. By tracing data flows and evaluating the security controls of external partners, you protect patient records and hold your compliance program together. A precise mapping protocol prevents incidents in a sector where a large and growing share of stolen patient records now originate from external vendors rather than the hospital itself.
This practice ties directly into the broader third-party risk obligations enforced by the Department of Health and Human Services (HHS) Office for Civil Rights (OCR). Under the law, covered entities and business associates share liability for supply chain breaches. In this article I explain risk analysis, security controls, data protection, and mitigation, then walk through a seven-step process. Drawing on 2025 and 2026 enforcement patterns and our delivery work across 6,000+ audits, I outline how to build an audit-ready supply chain program.
Why Vendor Oversight Matters in Healthcare
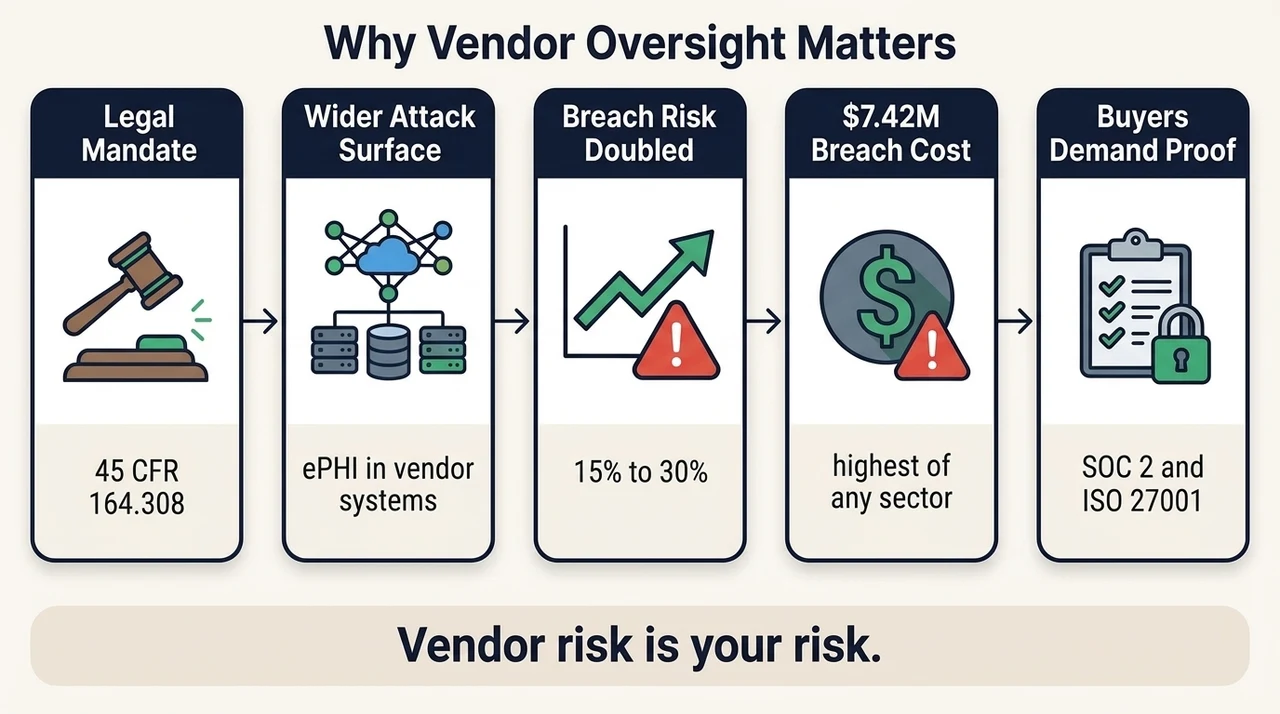
Vendors execute critical functions across healthcare. They supply cloud infrastructure, run revenue-cycle operations, process billing claims, and host clinical analytics platforms. Every third party that handles, transmits, or stores electronic protected health information (ePHI) expands your exposure.
Under the Health Insurance Portability and Accountability Act, third-party compliance duties are not optional. Covered entities must ensure their vendors implement adequate administrative, physical, and technical safeguards. The specifications live in 45 CFR 164.308, which requires organizations to obtain satisfactory assurances from their partners. This is a legal mandate, not a best-effort suggestion.
The consequences of weak oversight are measurable. The Verizon Data Breach Investigations Report found that third-party involvement in breaches doubled year over year, climbing from 15% to 30% of incidents, which shows how vendor weaknesses increasingly expose their customers. In healthcare that trend hits harder, because so much patient data now lives inside external systems. OCR's public breach portal records how often reported incidents involve a business associate rather than the covered entity alone.
Beyond regulatory fines, breaches cause operational disruption, erode patient trust, and stall enterprise sales. Industry analyses continue to place the average cost of a United States healthcare data breach at roughly $7.42 million, the highest of any sector.
When your sales team tries to close a hospital contract, procurement officers demand SOC 2 Type II reports, ISO 27001 certificates, and rigorous security addenda. The evidence that blocks or accelerates a deal depends entirely on your third-party oversight. If you manage vendor security in static spreadsheets, enterprise buyers will find the gaps during due diligence.
Core Concepts You Need to Understand
Before you execute a program, clarify the overlapping terminology. Confusion here leads to failed audits and delayed enterprise deals.
Risk Analysis vs. Risk Assessment
Practitioners often use these terms interchangeably, but under the law they mean different things. Risk analysis identifies the threats and vulnerabilities across your systems and external connections. It answers what could go wrong. Risk assessment takes that data and evaluates the likelihood and impact of each threat, then prioritizes the response using severity metrics such as the Common Vulnerability Scoring System (CVSS). OCR explicitly demands a rigorous risk analysis under the Security Rule.
Third-Party Risk Management (TPRM) and Vendor Security
Third-party risk management (TPRM) covers the full lifecycle of managing external parties, including financial stability and operational continuity. In healthcare, TPRM overlaps heavily with data-privacy mandates. A precise execution of HIPAA vendor risk mapping fits inside a broader TPRM strategy and acts as the security engine that guards patient records.
Essential Terminology
- Vendor onboarding: the intake phase where initial due diligence and security vetting happen before you sign a contract.
- Compliance assessment: testing a partner's controls against structured frameworks such as SOC 2, ISO 27001, or HITRUST.
- Audit trail: tamper-evident logs that prove system access, configuration changes, and data transfers over an observation period.
- Contractual safeguards: legally binding data-protection mandates, specifically Business Associate Agreements (BAAs) and Data Processing Agreements (DPAs).
- Security frameworks: established guidelines such as NIST CSF 2.0 or ISO/IEC 27001:2022 that provide the technical blueprint for control implementation.
Enterprise healthcare buyers will audit your vendors before they sign.
Drop your work email and we will turn your third-party risk into audit-ready evidence.
Step-by-Step Guide to HIPAA Vendor Risk Mapping
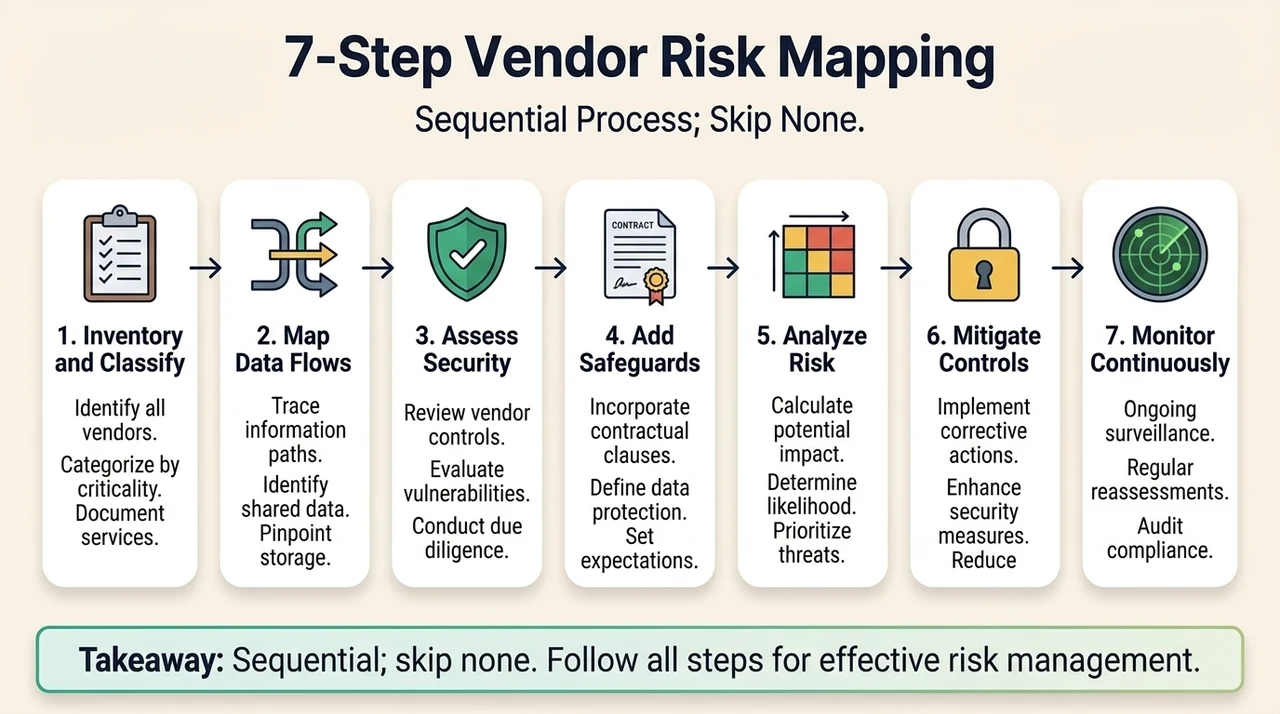
The process below is sequential. Skip a step and the gaps surface later, usually in front of a hospital procurement team.
Step 1: Vendor Inventory and Classification
Start by inventorying every external engagement that touches your systems or data. Most engineering teams badly underestimate their vendor count. Pull single sign-on logs, accounts-payable records, and procurement contracts to surface shadow IT. An exhaustive list is the only valid starting point, and it doubles as the front door for your secure vendor intake process.
Once identified, classify each entity by its interaction with ePHI, its operational criticality, and its technical access. A cloud host running your production database demands extreme scrutiny; a marketing analytics tool with zero access to patient records needs far less.
Prioritize the entities that pose the highest exposure for detailed mapping. This triage keeps your engineering and compliance hours focused on the infrastructure that actually stores or transmits patient data.
Step 2: Data Flow Mapping
Map exactly where ePHI enters, moves, is stored, and is processed inside external systems. This PHI data flow mapping is the foundation for audit evidence: if you do not know where data travels, you cannot protect it. Data flow diagrams (DFDs) are mandatory artifacts for ISO 27001 and SOC 2 audits, and they prove to enterprise buyers that you understand the exact boundaries of your Information Security Management System (ISMS).
Map the flow across specific availability zones, databases, and application programming interfaces. Document the encryption protecting data in transit, enforcing TLS 1.2 or higher on every path. Document the encryption at rest as well, ensuring AES-256 applies to all databases, object-storage buckets, and block-storage volumes.
Step 3: Conduct Vendor Security and Compliance Assessments
A vendor security assessment relies on structured controls checklists and real evidence; a self-attested document is never enough. Evaluate external controls meticulously against established standards. Check for strict logical access control, encryption, mandatory multi-factor authentication, and centralized audit logging. Review incident-response capabilities and disaster-recovery SLAs. A standardized security questionnaire keeps these reviews consistent across partners.
Score exposure by likelihood and impact. Require each partner to provide a current SOC 2 Type II report or ISO 27001 certificate, and read the auditor's observation period carefully. Study Section 4 of the SOC 2 report for exceptions in change management or access reviews. If the report shows control failures in the CC6 series for logical access, your patient data is at risk.
Step 4: Integrate Contractual Safeguards
A Business Associate Agreement (BAA) is legally required for any entity that handles ePHI on your behalf, but a business associate agreement is only paper if the technical controls behind it fail. Spell out the contract language during procurement. Mandate specific data-protection requirements and define exact technical controls. Set breach-notification timelines to 24 or 48 hours rather than the regulatory maximum of 60 days, and align them with your breach notification process. HHS publishes model language you can adapt in its sample business associate agreement provisions.
Include subcontractor flow-down clauses so your partner's own vendors protect your data too; managing that chain is its own discipline, covered in our guide to subprocessor management. Use these contracts to enforce risk mitigation, including the right to audit systems annually, and demand indemnification clauses tied directly to data-exposure incidents.
Step 5: Risk Analysis and Categorization
Combine your assessment results and data flow diagrams into a centralized matrix that shows what threats exist, where they originate, and how severe they are. Record the findings in a formal risk register so auditors and enterprise buyers can review them quickly. An organized risk map demonstrates that you actively watch your supply chain rather than reacting after an incident.
Categorize findings with a standard scoring model, such as assigning a CVSS score to each software vulnerability found in a vendor application. That consistency holds your TPRM program together. A critical vulnerability mapped to a vendor API must trigger an immediate incident-response protocol.
Step 6: Implement Mitigation Controls
Assign every mitigation action a strict SLA and a named internal owner. Apply compensating controls inside your own stack to limit exposure, and restrict external access to ePHI using least-privilege principles. Review AWS IAM roles and GCP service accounts so vendors hold only the permissions they truly need.
Increase automated monitoring on external API connections, and set contractual performance metrics that penalize partners for security downtime. Internal IT, legal, and compliance must coordinate to enforce these mitigations. If a vendor refuses to implement a necessary safeguard, terminate the contract.
Step 7: Continuous Monitoring and Reassessment
One-off assessments do not deliver real security. Controls that look good in a static document but fail under incident pressure are a liability. Continuous monitoring detects emerging threats and control degradation as they happen.
Define a strict reassessment cadence and evidence-refresh schedule based on each partner's risk tier. Automated tooling supports real-time alerts and tamper-evident audit trails, so your evidence never goes stale inside an audit observation window. Enterprise sales depend on your ability to show buyers that your controls operate effectively every day of the year, not just on the audit date.
Operational Realities: What Breaks in the Field
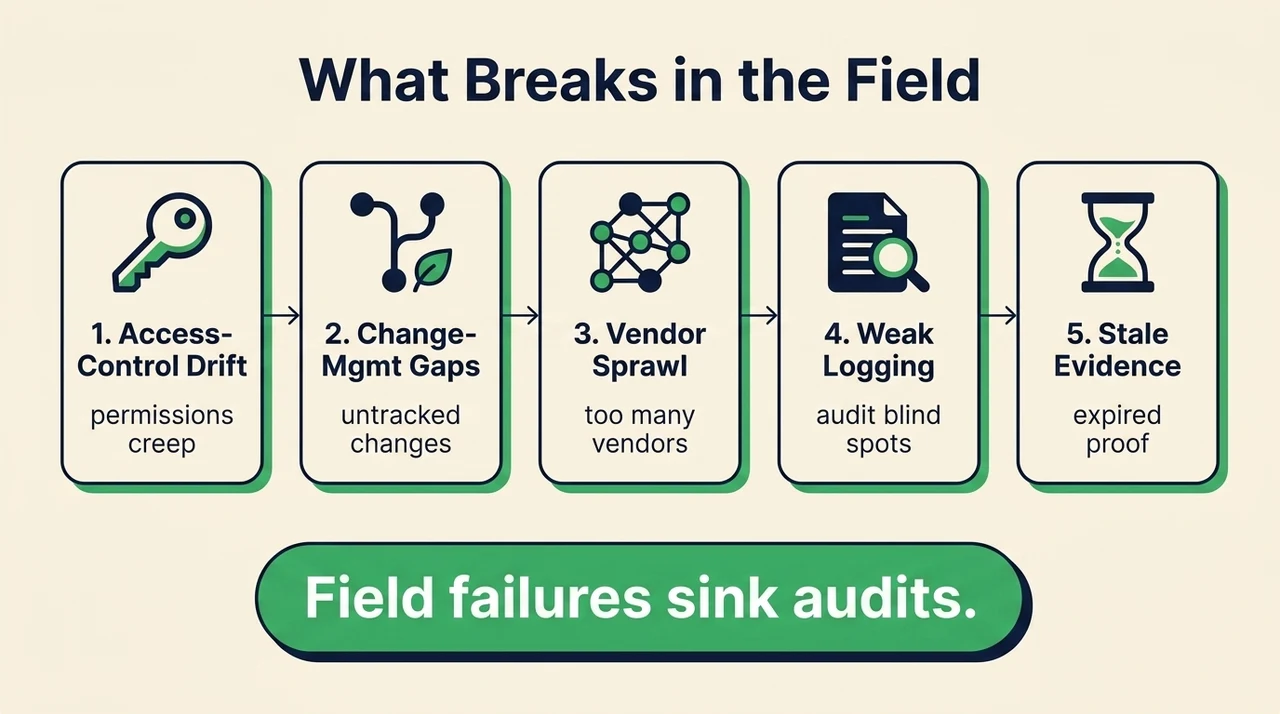
Across 6,000+ audits and 25+ years of combined technical experience, we see exactly what fails during due diligence. Access-control drift, change-management gaps, vendor sprawl, and weak centralized logging undo otherwise solid compliance efforts.
Evidence staleness during observation windows leads to qualified audit opinions. In healthcare specifically, the recurring pitfalls are ePHI exposure in lower staging environments, missing BAA signatures, and audit-log scopes that skip critical applications. Many teams configure their SIEM to watch the primary database but ignore the external data warehouse where their models actually process patient records.
When compliance fails, the financial damage is severe. In January 2026 HHS updated its civil monetary penalties for inflation; the maximum penalty for a Tier 3 willful-neglect violation now reaches $2,190,294 per violation. Ignorance of supply chain vulnerabilities offers no protection during an OCR audit.
Internal engineering teams burn hundreds of hours chasing partners for updated penetration-test reports and security certificates. Without an operationalized process, supply chain oversight becomes a constant drain, and teams slip into compliance manufacturing: generating artifacts to pass an audit instead of building real security.
Best Practices for Effective Oversight

Apply established security frameworks such as NIST CSF 2.0, HITRUST, or the SOC 2 Trust Services Criteria to structure your assessments and formalize your approach. Keep a tamper-evident audit trail of every assessment, acceptance decision, and remediation activity.
Maintain cross-functional governance across security, compliance, legal, and procurement, and wire these principles into your onboarding and offboarding workflows. When procurement requests a new purchase, the security review should act as an automated gate rather than an afterthought.
Require objective evidence over self-attested claims: configuration screenshots, exact password-policy settings, and live monitoring dashboards. Train both internal teams and external partners on privacy rules, incident-reporting expectations, and secure coding.
Tools and Frameworks That Support the Process
You need systems that track exposure, automate evidence collection, and keep audit documentation current year-round. Manual spreadsheets invite version-control errors and missed renewal dates.
Frameworks such as ISO 27001:2022 and NIST SP 800-30 provide structured approaches to thorough assessments; use them to standardize your controls and assessment criteria. Automation platforms that connect directly to your cloud infrastructure can pull real-time configuration data and verify that external connections remain secure.
Build dashboards that display live SLA adherence for vulnerability management. Track the percentage of critical CVSS findings remediated within 48 hours, high within 14 days, and medium within 30 days. Showing those metrics to auditors is direct proof that your program works.
Case Example: Charting a Vendor Risk Map
Consider a B2B SaaS platform that provides telemedicine analytics to large hospital networks. During procurement, a major hospital system asks for the platform's complete HIPAA vendor risk mapping documentation before signing a multi-million-dollar contract.
The platform hands over a detailed data flow diagram showing ePHI entering through encrypted APIs, processing inside an isolated AWS environment, and resting under AES-256 encryption. It presents a current risk register listing each of its own external partners, detailing SOC 2 Type II status and BAA execution dates for every one.
Because continuous monitoring is already in place, the platform instantly generates an evidence report showing zero high-severity vulnerabilities across its infrastructure over the last 90 days. The hospital's procurement team approves the security addendum in two weeks instead of the usual six months. The deal closes faster because the evidence is precise and verifiable.
A Durable Approach
Konfirmity delivers human-led, managed security and compliance. We provide an outcome as a service, executed by dedicated practitioners. We do not just advise; we do the work.
In our delivery experience, self-managed SOC 2 Type II readiness stretches across most of a year and pulls hundreds of hours from internal engineering. With Konfirmity, teams reach readiness in four to five months and spend roughly 75 hours per year of internal time. We implement controls directly inside your stack and run continuous monitoring, access reviews, third-party risk workflows, Data Protection Impact Assessment (DPIA) triggers, and vulnerability SLAs.
By mapping controls across ISO 27001, SOC 2, HIPAA, and GDPR at once, we remove audit fatigue. Start with security and arrive at compliance. Build the program once, operate it daily, and let compliance follow.
Conclusion
A rigorous HIPAA vendor risk mapping strategy is a requirement for data protection and regulatory survival in healthcare, not a one-time project. It is a permanent, daily function of third-party management. Start today by building a complete, accurate inventory of every external connection. Implement real controls, demand continuous evidence, and you protect patient data, satisfy enterprise buyers, and pass audits without the last-minute scramble.
FAQ
What Is HIPAA Vendor Risk Mapping?
It is the structured practice of identifying, categorizing, and continuously tracking the security posture of every third party that touches patient data, in order to safeguard ePHI and prove that external partners meet HIPAA's requirements.
How Often Should You Update Your Assessments?
Treat it as continuous. Require annual reassessments for high-risk partners, and trigger an immediate review on contract renewal, a major configuration change, or a security incident reported in the news.
What Is the Difference Between TPRM and Healthcare Compliance?
Third-party risk management covers all external risk, including financial and operational stability. Healthcare compliance specifically mandates technical and administrative protections for ePHI. Vendor risk mapping bridges the two.
Does Every External Partner Need a BAA?
No. Only entities that create, receive, maintain, or transmit ePHI on your behalf require a Business Associate Agreement. A solid risk map tells you which partners cross that line.
What Are the Most Common Vulnerabilities Found During Audits?
Weak logical access controls, missing encryption at rest, poor centralized logging, and absent subcontractor flow-down clauses in legal agreements.



